Article
What Is ISTDP?
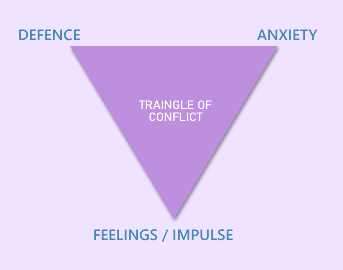
Intensive Short-Term Dynamic Psychotherapy (ISTDP) was developed by Dr. Habib Davanloo at McGill University in collaboration with Dr. David Malan, whose Triangle of Conflict and Triangle of Person are foundational to ISTDP.
Davanloo was concerned about the duration of psychoanalysis, its reliance on interpretation, and the implied omnipotence of the analyst. He created a modality rooted in the understanding that early childhood experiences lead to internal dynamics that develop as protective measures against feelings and impulses learned to be intolerable or unacceptable — but which later become the cage in which a person finds themselves trapped.
Dr. Ange Cooper states:
“ISTDP’s primary goal is to help the patient overcome internal conflicts to experience all of their true feelings about the present and past — feelings that have been warded off because they are either too frightening or too painful. The technique is intensive in that it aims to help the patient experience these warded-off feelings to the maximum degree possible; it is short term in that it tries to achieve this experience as quickly as possible; and it is dynamic because it involves working with unconscious forces and transference feelings.”
Which Client Concerns Is ISTDP Especially Effective With?
ISTDP is effective for anxiety, depression, and relational difficulties.
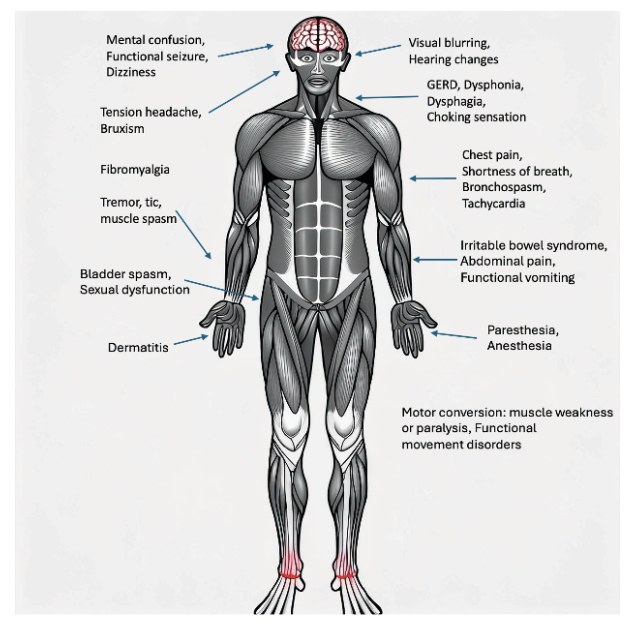
It is also supported for clients with C-PTSD/PTSD and treatment-resistant personality disorders, and has a strong evidence base for working with medically unexplained somatic symptoms.
How Does It Work?
ISTDP facilitates change through invitations to experience complex emotions connected to past attachments that underlie the issues clients seek help with. It involves building tolerance of unconscious anxiety and identifying and deactivating defenses.
We try not to get caught up in thoughts but are more interested in what lies underneath them.
For example, a client says:
“I don’t feel good enough.”
We invite them to see this as a defense, not a feeling. We don’t try to change or analyze the thought; instead, we invite them to get to the bottom of what it is defending against.
This process is known in ISTDP as “pressure.”
The client shares a specific relational example of when this defensive thought arose. Through a process tailored to their anxiety tolerance, they explore whether this thinking pattern emerges when interacting with people who don’t meet an attachment need and when feelings arise toward that person.
“I’m not good enough” may be functioning as a defense to cover up that truth.
When anxiety tolerance has increased and defenses have been sufficiently exhausted, those underlying true feelings may appear in the transference, and that is welcomed.
We then express curiosity about the links between those feelings and their original targets — the early caregivers — and the bodily experience of grief, rage, guilt, and love the client has been denying themselves.
The process tends to help people become more open and integrated. It’s relieving and freeing to get underneath the anxiety and defenses. It can feel like diving for a treasure chest — hard work, but well worth it.
What Do You Like Best About ISTDP?
Kim Boivin-Sonolet (KBS):
“I was initially inspired to explore ISTDP first as a client, then professionally. I’ve been using ISTDP since 2017.
I most appreciate the emphasis on us being attachment-based creatures with needs that create feelings in our bodies. When these needs are not met — especially by people important to us — we may unconsciously engage a combination of bodily anxiety and defensive processes to avoid the powerful mix of feelings and impulses that arise.
This way of looking at the human condition and the symptoms people bring to therapy is foundational to ISTDP. I find it a grounding, humanizing, and compassionate way to work.
I’ve had more moments of deep emotional connection with my clients; I feel more emotionally open and have seen that transformation happen in them as well.
I also love that clients can apply Malan’s Triangle of Conflict and Triangle of Person to navigate challenges in their lives. They don’t need to rely on me — it’s collaborative and empowering.”
Robert Bal (RB):
“I became an RCC specifically to practice ISTDP after a significant experience with it as a client. I view it as inherently compassionate — an active attempt to reach the person inside the person, the one who was long ago locked away.
What I most love is the way it centers the unconscious.
I am continually awed by how the unconscious moves in therapy — how, in this relational work, there is the unconscious of the client, the unconscious of the therapist, and then, as attachment develops, an unconscious therapeutic alliance — an active healing force leading the dyad forward.
This force can perhaps be understood as the sound of that same music toward which spirituality and faith the world over are directed.”
Are There Other Modalities It Pairs Well With?
ISTDP is inherently trauma-informed and pairs well with any modality used with trauma survivors.
It shares similarities with aspects of CBT, particularly regarding views of self and other. The Rogerian foundation upon which most good therapy stands is also consistent with ISTDP.
ISTDP and EFT (Emotion-Focused Therapy) both emphasize attachment, emotions, and negative interactional cycles. AEDP (Accelerated Experiential Dynamic Psychotherapy) was developed by Diana Fosha, who trained with Davanloo.
The relative cost-effectiveness of ISTDP — linked to shorter treatment durations — means it has potential value for marginalized clients who face barriers to therapy, and it connects naturally with multicultural and feminist modalities.
Are There Any Issues ISTDP Should Not Be Used With?
According to the ISTDP Institute:
“Other treatment options should be considered for patients suffering from organic syndromes, brain injury, active psychosis, active alcohol and/or drug addiction, severe acting out, antisocial personality disorder, and life-threatening active health conditions (e.g., active inflammatory bowel disease).
For some disorders, ISTDP might be considered if the patient’s condition has stabilized (e.g., bipolar disorder, some psychotic conditions), but these should only be attempted with great care and advanced training.”
Where Can We Learn More?
There are many opportunities to learn ISTDP!
Core trainings are offered by instructors who trained directly with Davanloo, such as:
-
Dr. Allan Abbass
-
Dr. John Rathauser
-
Dr. Patricia Coughlin
Many from the following generation have also become trainers, including:
-
Dr. Joel Town
-
Jon Frederickson
-
Dr. Jonathan Entis
Shorter trainings with specific areas of focus are also available.
Much ISTDP literature exists, including Davanloo’s original texts, Abbass’s Reaching Through Resistance, and Frederickson’s Co-Creating Change.
Finally, it is our heartfelt recommendation that one of the best ways to learn ISTDP is to experience it first-hand — as a client.